
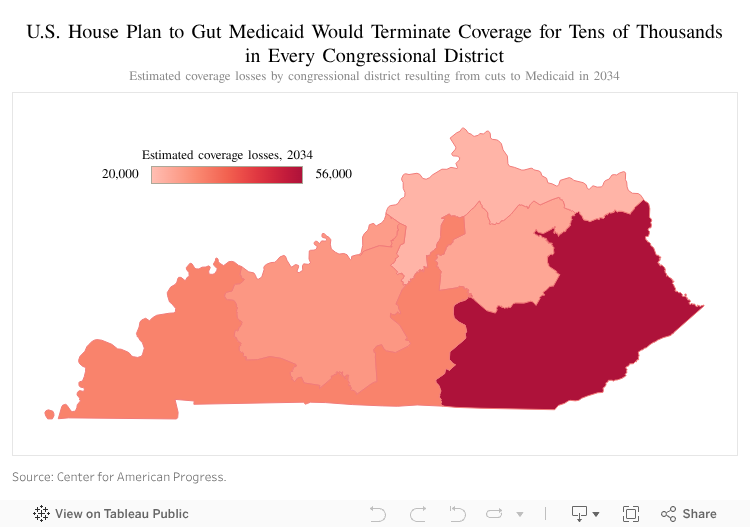
The United States House of Representatives has passed a plan to reduce Medicaid spending by an estimated $1.7 billion for Kentucky, terminating health coverage for as many as 345,000. Kentucky would see the second largest cut proportionate to our Medicaid program, and see the fifth largest coverage losses outright. Nationally, it would lead to an estimated minimum of 8.6 million losing Medicaid and marketplace coverage and becoming uninsured according to the Congressional Budget Office – other estimates are even higher. These coverage losses would be in addition to an estimated 47,000 Kentuckians who would become uninsured due to the failure to extend the enhanced subsidies on kynect, the health insurance exchange. These would be the biggest, most severe cuts in Medicaid’s history.
Kentucky has made great strides in its health and economic wellbeing since implementing Medicaid expansion in 2014, making Kentucky among the states most at risk from the cuts to the program laid out in the House budget proposal. Terminating coverage and making care more difficult and expensive to use would reduce health and weaken our economy. The House bill would eliminate jobs, especially in rural areas, damage our progress tackling severe problems like addiction and even lead to lost lives. The U.S. Senate will now pick up the legislation to consider its approach to Medicaid, taxes, and other vital programs – it must reverse these grievous and extreme cuts.
Terminating coverage for certain adults who don’t adequately report work hours
The first way the plan would terminate health coverage would be by requiring adults ages 19-64 who do not have a documented disability or a child report at least 80 hours of work (or other qualifying activities) each month. Such work reporting requirements have been highly effective at taking away benefits in programs like SNAP, but have no meaningful record of improving employment or wages. One estimate shows anywhere between 120,000 to 136,000 Kentuckians, including people with disabilities and serious health conditions, could have their health coverage terminated from getting tripped up by this paperwork requirement. Research suggests that this population is disproportionately comprised of women, those with a high school education or less (and therefore less likely to qualify for many jobs), people who have recently left the workforce, or those who are out of the labor force caring for an adult child or aging loved one (not children, which would otherwise exempt them from the requirement).
Two states have implemented such a requirement for Medicaid with terrible results. In Arkansas, 18,000 people lost coverage before a federal judge put a halt to its program. In Georgia, over 200,000 otherwise eligible adults have gone without health care coverage due to these requirements, with under 5,000 qualifying due to the complicated and burdensome reporting rules. In both of these cases, developing the unwieldy technology and administrative structure to enforce the requirement was very expensive.
Additionally, it is likely that the complicated reporting aspect of this requirement would lead to the majority of terminations, not the inability of Kentuckians to work or otherwise be exempt. Over half of Kentucky adults covered by Medicaid already work, mostly in low wage jobs that do not offer health care. This often-unsteady work can come with unpredictable hours and lack of sick leave, making it especially difficult to meet reporting requirements when hours are reduced or during illnesses. Of those on Medicaid who are not working, all but 2.3% are either ill or disabled, taking care of a loved one, retired or actively seeking work.
This policy would have a large negative impact on the economy as well. With so many fewer people seeking care paid for by Medicaid, one estimate suggests Kentucky could lose up to $1.3 billion in federal funding, leading to as much as $98 million less in state tax revenue and up to 12,100 fewer jobs (nearly half of which would come from outside the health sector).
More frequent eligibility checks that will trip people up
Another policy in the House plan aimed at cutting Medicaid costs is to increase the number of times people who are covered under the Medicaid expansion must prove they are eligible. The plan increases that requirement from once per-year to every six months, with the assumption that many people will err in their paperwork or take too long and then lose their coverage. This assumption is not unfounded – during the “unwinding” of the COVID-era coverage protections, anywhere between 15.1% of enrollees had their coverage terminated due to “procedural denials,” which simply means they lost coverage not because they were ineligible but because their paperwork was wrong, late, or missing.
Currently, adults only submit for re-enrollment once per year, and many are renewed automatically because of existing data sources that confirm their eligibility on their behalf (often called “ex parte” renewals). In between renewals, however, they must report if their circumstances change such that they would no longer be eligible for coverage. Increasing the paperwork, as proposed in this bill, changes this long precedent, and will certainly lead to large coverage losses.
Copays that will discourage the use of care
Under the House plan, enrollees with incomes over 100% of the Federal Poverty Level (FPL, or $15,650 for an individual) would have to pay mandatory copays when receiving care. Copays would be capped at $35 per service, and the out-of-pocket maximum would be 5% of income. For an individual at the poverty line, that could mean copays of up to $783 per-year out of an already unlivable wage.
Copays are designed to save money not by recouping part of the cost of the care (which dwarfs the value of the copay), but by discouraging the use of care to begin with. Applying that disincentive to the lowest-paid Kentucky households would have an even greater effect as their financial margins are very tight. In that way, care would likely be delayed until the condition worsens and becomes more expensive and difficult to treat. Imagine a woman who notices a lump, but refuses to get a mammogram until it has grown very large and possibly metastasized, or someone who has dizzy spells but waits to see a cardiologist until they’ve had a heart attack because they had no financial cushion with which to cover a copay until their condition is desperate.
Medicaid is a health coverage program that is designed, in part, to encourage wellness by reducing barriers to care. Managed Care Organizations hire Community Health Workers, provide value-added services, and offer healthy behavior incentives to foster increased preventive screenings and treatment. Adding a financial barrier to that care works against that goal.
Other ways the plan seeks to cut Medicaid
There are several other more technical changes that would contribute to loss of coverage and other forms of cuts to Medicaid. One is the repeal of a Biden-era provision known as the “eligibility and enrollment” rule, which is designed to smooth the way to getting enrolled in Medicaid and then make it easier to stay enrolled. This repeal alone would terminate Medicaid coverage for 2.3 million Americans. The majority of those losing care would be dual-eligible enrollees, meaning they are people with a disability or retirement-age who are also covered by Medicare but have incomes low enough that they qualify for both programs. The result would be significantly higher health care costs for some of the most medically vulnerable people. In Kentucky, 175,300 are dual-eligible.
Another change would prohibit the increase or creation of new provider taxes, which are often used to offset the state portion of Medicaid costs. This could later put financial pressure on Kentucky’s Medicaid program, leading to cuts in Medicaid or other programs paid for by state government to offset the increased cost.
The proposal also reduces what is known as “retroactive eligibility” from 90 days to one month. Retroactive eligibility is a policy that allows a provider to be paid for the care they provide up to 90 days before someone becomes eligible for Medicaid. This rule exists because it can often take states more than a month to process an application. The federal government currently requires that standard applications be processed within 45 days, and those with a required disability determination must be processed within 90 days. In expansion states like Kentucky, over 20% of applicants wait more than 45 days for approval (though Kentucky has a good record of speedy determinations for most applicants). If someone is determined to be eligible, retroactive eligibility is designed to pay doctor bills while their application is being processed. Shortening that period makes it more likely ill Kentuckians will face huge medical bills and may make providers less willing to offer care prior to coverage.
The depth of the coverage losses is even larger because of reductions in marketplace assistance
Another significant cut that will harm the health care of thousands in Kentucky is being proposed in a separate committee (Ways and Means). By omitting the extension of enhanced subsidies to individuals and small businesses who must purchase coverage on kynect.com, health care prices will spike by thousands of dollars, and an estimated 57,000 will lose subsidies and 47,000 of them would be priced out of health insurance altogether, especially middle-class households that do not receive coverage at work. These subsidies have been helping many thousands of Kentuckians afford coverage since 2021 and allowing them to expire will make it even harder for those who lose Medicaid (among others) to afford a doctor or medicine.
Terminating coverage and reducing care would move us in the wrong direction
Together, these policies comprise the largest spending cut to Medicaid in the history of the program, larger than all previous Medicaid cuts combined. As a state where more than a million people rely on these vital federal programs, Kentucky would be left sicker and poorer by these cruel and unnecessary changes.
New paperwork requirements from increased redeterminations, the repealed “eligibility and enrollment” rule, and mandatory reporting of work hours are all designed to cull the number of people with health insurance. Copays are a cruel barrier for those who can keep their coverage, forcing already struggling families to jump one more financial hurdle in order to receive needed care. And making it more difficult for states to pay for Medicaid, or for hospitals to accept it, will put increased pressures that will ripple outside of Medicaid and cost lives and livelihoods alike.
Updated: May 22, 2025



